

DXB
-
Posts
3,551 -
Joined
-
Last visited
-
Days Won
13
Content Type
Profiles
Forums
Blogs
Gallery
Downloads
Media Demo
Events
Store
Everything posted by DXB
-
Active infection and history of infection require two separate types of tests - these are generally done with detecting viral RNA in the first case and serum antibody in the second. Both types of tests have imprecision, making interpretation particulary difficult in populations where the condition being tested is not very common. Then there are multiple flavors of both types of tests - for antibody tests the two varieties were described well by @bradp above. A negative test for an active infection - does that indictate immunity? That is a subtle question - as RNA goes down the antibody generally comes up. The ability of RNA tests to detect infected people starts to decline right after symptom onset, except in the people who will get scary sick in the second week. The antibody tests (particularly the IgM component) will identify some of those diagnoses in sick people missed by RNA, as will CT scans of the chest. Then there is the question of how reflective serum antibody is of immunity, and how much of that immunity is a direct result of the antibody - that answer is coming, but it may some time. The implications for vaccine development are profound.
-
Ross - thank you - that is an overly kind assessment. My communication style is a work in progress and a byproduct of a couple of decades spent being an arrogant ass, wondering why I wasn't all that great at solving problems. I suspect some others here have progressed much faster in that regard.
-
No insult intended at all here and sorry if I came off as patronizing at any point...to keep the discussion going in a productive direction, and to address the key points you raise (we are less far apart here than you might imagine): "We are making a huge reaction to projected outcomes when we still don't have a denominator as to how many people have had this virus suffered minor symptoms if any and moved on." That is undoubtedly true - many early estimates of mortality were badly inflated by low testing. The problem is that at the moment the estimates at the very low end may have an artificial inflation of the denominator. The reason is that tests in populations that have a low prevalence of the condition that is being tested, be it active infection or protective antibodies indicating prior infection, will produce a very high proportion of false positives. Take the extreme example: a population where no one has truly has had the virus. Let's say you have a serum antibody test with 95% specificity and specificity - that is a pretty good test and on par with the first FDA-approved serology test. If you test an infection free population, 5% will test positive, but they will all be false positives - sounds pretty close to the numbers in that county in CA right? There could be other explanations for sure - a less virulent strain, or more immunity than predicted by initially reported cases, but the innate limitation of the test is the first thing that comes to mind. "I also am VERY suspicious of the number of deaths that were strictly due to the virus and not underlying conditions" There is no question that other conditions contributed to the tallied deaths from COVID19. First there are innate imprecisions in reporting, but these errors tend to go both ways (e.g. the false positive COVD19 test in the person actually dying of influenza vs. the old person found dead at home of unknown causes). It's hard to make out if there is a large net error in one direction or the other. The people ending up dying in the ICU after a positive test for the virus overwhelmingly are older and have other medical conditions. Some of them have medical conditions so serious that they have very short life expectancies even if they didn't catch the virus. But lots of others have life expectancies measured in years to a decade or more. Consider the 70 year old male whose hypertension and diabetes are under medical management. Even though he takes care of himself and is active in his retirement, he is quite vulnerable to die of the virus despite having years of life expectancy - should we not count him in the numerator and do all we can to help him? We would do everything for him if he showed up with heart disease or a treatable cancer, so I have a hard time dismissing him as a illegit COVID19 statistic who was going to die anyway of something else. "I guess all the millions of normal hard working people that are in the process of losing everything should just keep their uneducated mouths shut" They should not keep their mouths shut. The economic impact cannot be ignored. I am far less qualified to speak to those issues, and neither are most of the people belittling their urges to restart the economy.
-
if she gets sick, her chances are not good - obesity is a major risk factor for mortality. So keep your social distance Chris - you don't want that "weighing" on your conscience
-
Here's a "fun" visualization of the dynamics of COVID19 mortality increases through mid April. Of course the comparison categories for mortality shown are historical averages, not real time data, but it's certainly one useful window into understanding the virus' impact. .https://public.flourish.studio/visualisation/1712761/?fbclid=IwAR05Gqc3d2F9kd2qdcqv25hVZJI0lnU0LsPcqMRm-jPsiJwpSnJq7kWgRCk At the risk of sounding callous, it's not the only relevant way to look at mortality here. Another one might be life expectancy years lost from a disease. By this metric, the accidents and overdoses etc. might still dominate given the strong bias of COVID19 mortality toward older people with medical comorbidities.
-
Some related comments on viral mutations, mechanisms of immunity, and hospital capacity: - There is antigenic drift seen here as with any rapidly replicating pathogen, but really not that much in relative terms (e.g. the early days of HIV). This virus has found a rare adaptive niche in humans in a manner that occurs only every 100 years - i.e. very high transmissibility combined with fairly high pathogenicity. I suspect this virus won't have much ability to change and still maintain that rare combination of features. Certainly mutations allowing antigenic escape will happen as more of the population gets exposed and/or we widely apply an effective vaccine. But I suspect such changes will also knock this virus out of that special ecological niche. Mutations hurting transmissibilty will be strongly selected against of course. So I suspect any such changes will sustain transmission but attenuate pathogenicity, which may prove tantamount to the virus going away. - The mechanism of protective immunity is not a trivial question, particularly as we roll out all these serologic tests and try to develop a vaccine - the test may directly measure the antibody protective mechanism, strongly correlate with a cell-mediated protective mechanism, or unfortunately correlate poorly with effective T memory. We're all kinda hoping humoral immunity works here, but really I don't know enough about coronavirus immune responses to say. I don't think the killed whole virus and recombinant spike protein approaches to SARS-CovV were all that effective, which is a little ominous. Maybe the fancy liposomal DNA and RNA-based vaccine techologies will fare better here, but they don't have a proven track record of efficacy. I worry we will need a very strong driver of cell mediated immunity like the recombinant live VSV-based Ebola vaccine, which worked quite well but had a side effect profile that would make application to the entire population challenging. I'd love to hear more from vaccine experts on this. -The flip side of protecting hospitals from being overwhelmed is providing the pressure to expand capacity under a deluge of patients while government steps up to bat to support that effort. Presently we have tried to expand capacity for COVID19 patients at great cost to normal hospital operations, and much of that capacity around the country now sits unused. Under these conditions, hospitals are hemmorhaging money, and many patients can't get elective care or choose to delay addressing urgent problems so they don't have to go near a coronavirus-infested hospital. Unfortunately getting past this unsustainable situation, particularly if a good vaccine is likely to be hard, may be to open the floodgates on transmission more than makes us comfortable. Only then will we see our true ability to handle the deluge, and we will have an economic engine in the country still functioning to help us do it, unlike what we have now. Remember we are the country that expanded its military from 500k to 12 million in the years following Pearl Harbor out of dire necessity - that would have seemed impossible before that. We can do something similar for ICU care. The care quality may not be on par with that in the MICU at MGH, but it doesn't need to be. We are saving less than half of ICU admits with this disease at present anyway, and most of that survival can be preserved under the kind of pressure that drives resourcefulness. And the volume of clinical experience will also settle a lot of the questions presently on how to care for these patients (e.g. should it truly be managed like ARDS in some cases) and ultimately improve outcomes.
-
1) Should I forget the asterisk and just lean until I feel a stumble in the engine, note that setting on the gauge and then richen a few notches on the gauge? YES!! Or if you have fuel flow, just use that instead of the EGT gauge. You'll find it more reliable. 2)I ultimately want to get an engine monitor and that will be my next mod but I don’t currently have one. Definitely do that - it is a terrific diagnostic tool and safety feature...sadly on a carb'd bird it doesn't help leaning much more than the lean to rough/rich to smooth method. 3) And the concern is above 65% power, right? Can someone help explain the red box and also share their leaning procedure for the C, please? Mike Busch's EAA seminars and books explain in some detail. Bottom line on the 180hp O-360 is that you're pretty safe leaning under 75% power. The concern is greater on higher power to displacement ratio engines, with 65% power a great rule of thumb in those cases.
-
Thanks Andy - hope you feel better soon - the "good" news is that everyone is still getting all the other seasonal respiratory infections and allergies normally floating around, so chances are better than not that you don't have it. I ain't doing squat in terms of patient care right now by the way It's not bad enough in Philly that any MDs need to get repurposed, and the hospital is rather desolate. My usual cancer patients are mostly hiding, likely too afraid to go anywhere near the hospital, and all the elective care is canceled. There will likely be a deluge of work on the other side of this...
-
I am highly skeptical of data for any virus-naive population containing a normal age distribution reporting mortality under 0.5%. Note that aggressive testing of asymptomatic and mildly symptomatic people in a low prevalence population would falsely reduce the death rate , because most of the test positives would be false positives (that Bayes Theorem prediction). I could see some places getting caught up early obsession over "not enough tests" and pushing hard to apply the PCR test to everyone with the sniffles. That kinda seems like a California thing to do. *Another possibility is a less virulent strain taking hold in that population, but that seems less likely.
-
The part that makes me detest the Chinese government is their obsuring case numbers and death rates, and continuing to do so to this day. There were epidemiologic models built upon their published data early on that were used to guide subsequent decision making worldwide. That's where they unforgivably let the world down. Bureacratic inertia in the face of a new unfamiliar problem is almost expected (note we had plenty of our own), and I could care less if someone ate a bat (i imagine they're gonna stop doing that now). The biology behind why bats seem to harbor so many viruses that prove much more pathogenic in other mammals is fascinating btw, but I digress...
-
The worry is the ICU admissions and deaths. Of those 20% getting admitted to the hospital, only about 1/4 land in the ICU. The other 15% are quite easy to take care of - they are mostly there for supplemental oxygen and to be physically positioned for ICU admission and intubation should they need it. That capacity can be ramped up quickly. It's the vents, complex monitoring, clinical expertise in the ICU that are hard to expand - ICU care is an order of magnitude more resource intensive. Note death rates in the ICU if you get intubated are well over 50% even with the best care, so you are saving less than half the people who make it that far. Also note that hospitals nationwide are far emptier than normal, except in a few hotspots like NYC. Hospitals are like the airlines - used to running at near capacity to be profitable in an industry with very high overheads. They don't have an economic model for cancelling all elective care and sitting there with unused capacity waiting for COVID19 patients that may never come - it is pushing them to the edge, and it will change the industry forever. I agree with you completely about the inevitable fall spike in cases in a population with effectively no immunity. A lull in the summer is certainly possible but I am not totally confident it will happen.
-
A couple things worth poking with a pole here . The actual CFR in an average population of typical age and comorbidity distribution, and access to ICU care, is 1%. I would be willing to wager that, allowing for a 50% confidence interval on either side. The calculated ones are consistently higher, and with wide range, because of variation in how many symptomatic people are tested and the innate untestability of the asymptomatic pool (the latter requires a deep dive into Bayes Theorem to explain). Given that 1% mortality, Fauci is spot on in saying it is 10x more lethal than seasonal flu. Think of each case as having 10x more overall impact than a seasonal flu case - 10x more hospital admissions, ICU admissions, and deaths. Seasonal flu will never be a fair comparison here. Of note, if we had zero ICU beds, mortality would go up to 1.5% to 2%. The ICU is were people die of this disease if they come to the hospital, and optimal ICU care saves less than half if they land there.
-
A few apolitical comments about immunity - this is one of the most widely misunderstood concepts in the public dialogue: -At the individual level, immunity is never black or white - there is no such thing as total, perfect resistance to a pathogen for anyone, whether it's from a vaccine or from the natural infection. -Population level resistance (what we really need - the herd concept) does not require strong immunity or even durable immunity at the individual level. It merely requires enough resistance to the types of infections that produce a lot of virus shedding. The point is for there to be less pathogen in the environment. -That population level resistance is very likely to be achieved here with widespread enough infection, or the right vaccine, even if individual resistance to infection is fairly modest. -Will this virus mutate quickly as an immune escape mechanism? Luckily it appears fairly stable so far - we know it is a rather efficient beast that is well adapted to rapid spread, and so it may not be encountering much selective pressure early on. It will certainly change over time under immune selection pressure as more people are exposed and/or a vaccine is applied. There's a good chance those changes will also attenuate it's pathogenicity, reverting it back to being more like a common cold virus. I could not agree more that policy needs to be agile here as more is learned - the scientific knowledge is increasing exponentially along with the virus, though enormous uncertainty remains. At the same time, leaders are faced with a need for clear, coherent, and consistent messaging to the general population, which is not at all easy under these circumstances.
-
Ah - 2-4% That's right in the range I'd expect for an average population in the US. Considerable error in that measurement derives from variable sensitivity and specificity of that assay, and the multiple competing serologic tests in use at the moment, making it hard to compare directly to other populations (e.g. NYC, which I'm guessing should end up like 10%). The point is the numbers are all quite small and should confer negligable population level resistance.
-
Unfortunately that dip switch requires removing the surefly to access it...
-
I'd be interested to pick apart the first piece of data if you can post it. I agree with the second statement fully...
-
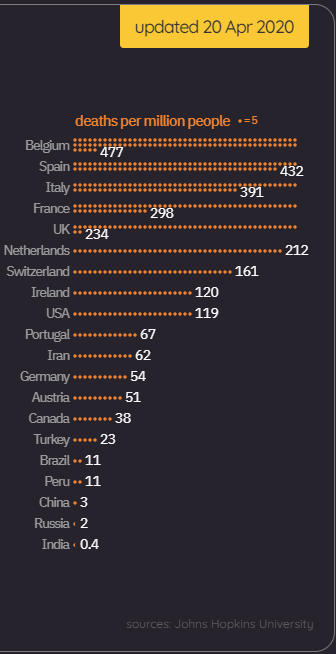
I find deaths per capita to be the single most informative statistic. Comparing total cases among countries, states, or cities is meaningless. And # positive cases is so sensitive to both the number of cases being tested and the testing criteria in any particular population. Death reporting is still error-prone, and in a few places it is complete BS (e.g. China and Russia), but it is probably the best comparative data we have right now. Will the places that had the fewest deaths early on be in the best shape going forward? I seriously doubt it - those deaths are closely linked to total numbers of cases and immunity in the population. Note where the US sits right now in the global scheme of things. I predict this will be over for Belgium, Spain, and Italy long before it ends for us. I would estimate 20% of Belgium's population has already been infected and has some immunity, vs. a paltry 5% for us.
-
A lot to unpack here in your comments, some of which I agree with. But as a PhD immunologist and a physician, I can say this one point is almost certainly false - the lower incidence in CA almost certainly stems from earlier, more aggressive government action, and possibly warmer temps. Once we have a reliable test of humoral immunity (it is a mess right now but will get better), I think we'll find that far less than 10pct of people in the US in any population, typically more like 2-5pct, shows evidence of prior infection after the first spike of cases. That is a huge problem in my view - no where near the 70% typically cited as necessary for herd immunity, and no easy way to get there without accepting either huge number of deaths or economic devastation until we have a vaccine. Unfortunately we are only in the first inning of this horrible game. Will CA be best served in the end by their faring better early on? I have little cofidence that will be true.
-
May I suggest a bottle of whiskey would be better if you need a liquid to serve double duty as hand santizer and helping forget all your problems. The effects on mental acuity reverse themselves a bit faster
-
YIKES CAREFUL ROB! The lipophilic nature of tetraethyl lead in leaded gas makes it an unusually efficient way to get lead through your skin, into your bloodstream, past your blood-brain barrier, and into the central nervous system components most effected by lead toxicity. I know there's plenty out there who use it to cut the grease off their hands in the shop, but it's a terrible idea. I don't stress too much over a small splash when sumping, but personally I'd rather take my chances with the virus if the only alternative was to rub 100LL into my hands as sanitizer. https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/tetraethyllead Incidentally I was searching for the same info about flight reviews when I found this thread. Mine's due in June - hopefully this situation will shake out a bit by then, but I'm not counting on it. So far I've managed to go out of my way to keep IFR current in actual - which is always a challenge.
-
Can't say I fully share the sentiment, but I did keep my SOS and wiring in place after my Surefly install. I'm still hoping my humility doesn't pay off
-
Boy this is a spectacularly interesting thread for a fellow Surefly early adopter and C model owner. I have a left Surefly, and I've had much higher #4 temps on takeoff whose cause still eludes me - though it's not as terrible as for @ragedracer1977. It ain't the fuel flow (always 17-18 gph at takeoff). It ain't the baffling - I've meticulously brought mine up to snuff over years. It ain't the timing - I was sure that was it because it coincided with the #4 problem appearing (overhauled R bendix mag was installed a couple months after the Surefly), but I had the R side tuned up to no effect. Oddly the hot #4 problem is there only during climb and low altitude cruise and goes away in high altitude cruise, where #2 goes back to being the problem child, like it's always been. It's like the Surefly is advancing at low altitude and high power, when it shouldn't. Mine doesn't run rough on the left side though. Maybe I have a minor version of the same problem?
-

Tower not answering - what actually happened here?
DXB replied to DXB's topic in Mooney Safety & Accident Discussion
Several good points made in the discussion here - thanks for letting me process a situation unfamiliar to me. Given the significant turbulence and my related fatigue, fumbling with my cell phone call might not have been the most effective thing to do, particularly since the tower number wasn't listed in the AFD - I had to call my FBO once on the ground to get it. I certainly thought about contacting approach while in the air; had the conditions been pleasant rather than turbulence in cold rain 1000ft below the freezing level, I probably would have done just that. Instead I was just fatigued and was still wondering if it was my screw up somehow - I just felt like being on the ground at that moment and took the easiest out. Calling ground or clearance frequency at the field would have been a great idea; unfortunately that only occurred to me once I landed at a nontowered field - another sign of my slowed mentation under the circumstances. I'm not interested in going after the controller here, though a NASA report would be reasonable. I do wonder if there is some increased complacency at ATC facilities seeing very little work during the COVID19 shutdowns - at least that was my first thought after not getting an answer from the tower at a field where I've landed many hundreds of times without issue. -
So I was flying back to my home field KPNE ( a large moderately busy class D under the Philadelphia Bravo) early this evening VFR without talking to anyone. Temps are dropping, and there is light precip and moderate turbulence. I am flying low to stay out of icing temps and am a little bit anxious to get home. I call tower from the southeast 12 miles out - no response. I then make repeated calls from both radios - nothing. Before reaching the class D boundary, I turn away and head for the nearest nontowered field ( KVAY) feeling very flustered. When asking for a radio check on CTAF, I get an immediate "loud and clear" and then enter the pattern and land. On the ground, I'm wondering if I missed the notam saying tower is closed because of low traffic volume during the quarantine, or the frequency changed, but that doesnt appear to be the case. I call the tower and tell the controller what happened. She says there is no issue with the frequency. I ask when was the last time she talked to anyone on tower frequency - she says two hours ago. I ask her again to check if the frequency is working. She comes back a few moments later and says something like "oh, sorry - it wasn't working, it should be ok now." I take off in worsening visibility and rain for the 5 minute hop and land uneventfully. I've no clue what it's like to work on the ATC side, but can anyone conjecture what actually happened here? Did someone fall asleep on the job after accidently flipping the wrong switch? I wonder how many other calls she missed. Should I have done something differently on my end under these circumstances? If I'd been on an instrument approach I could have leaned on the approach controller for help. I hesitated to call approach in the air here because I wasn't even on flight following , and I was wondering if the messup was actually on my end.
-
I think it's just RPM and MP. Base timing is set based on the DIP switches in the unit, as per specific STC parameters related to the engine. Mine is 25BTDC as is OPs, so advance may come at lower MP/RPM combinations. It's worth noting Surefly stopped publishing advance curves, and this one was meant to be conceptual, not precise for any particular engine.


